There are a number of different types of glaucoma. The commonest type of glaucoma is ‘chronic’ or ‘primary’ glaucoma. This is damage to the nerve of the eye that can be reduced by lowering the pressure within the eye. A less common type is ‘acute’ or ‘angle closure glaucoma’. This is a sudden massive elevation of eye pressure that causes sudden pain and loss of sight.
Chronic Glaucoma
Chronic glaucoma is poorly understood. It was originally thought to be high pressure in the eye that damages the nerve and sight of the eye. However, glaucoma can also occur at normal levels of eye pressure, known as Normal Tension Glaucoma.
Chronic glaucoma then is best defined as an optic neuropathy of unknown cause that damages the optic nerve and sight of the eye. This damage can be reduced or prevented by lowering the eye pressure.
Glaucoma is actually one of the commonest causes of blindness in the UK. This is because glaucomatous damage occurs without symptoms. Often, by the time a person is aware of visual loss, the disease is already very advanced, and the damage is irreversible.
Glaucoma has a number of risk factors, such as having a family history, increasing age, having afro-carribean descent or thin corneas.
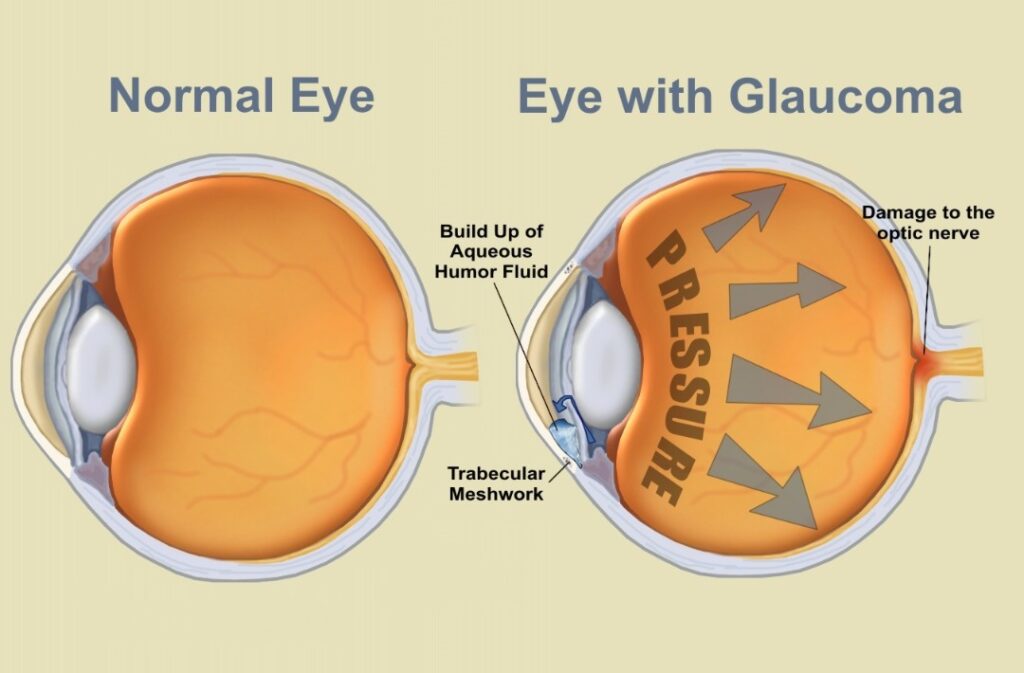
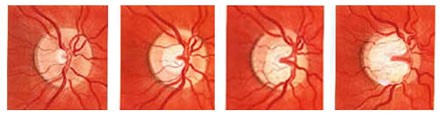
The damage to the optic nerve is often described as optic nerve ‘cupping’ or nerve fibre layer thinning. These are one and the same thing. When the nerve is healthy, it has a thick layer of nerve fibres connecting the eye and brain. As glaucoma damage occurs, this layer thins. This thinning can show itself as a hollowing of the centre of the nerve termed cupping, or a thinning of the nerve fibre layer coming from the retina and exiting the eye through the optic nerve.
The health or thickness of this nerve fibre layer can be measured by ocular coherence tomography (OCT or GDx). These can be found in some optometrist practices. An example is shown below.
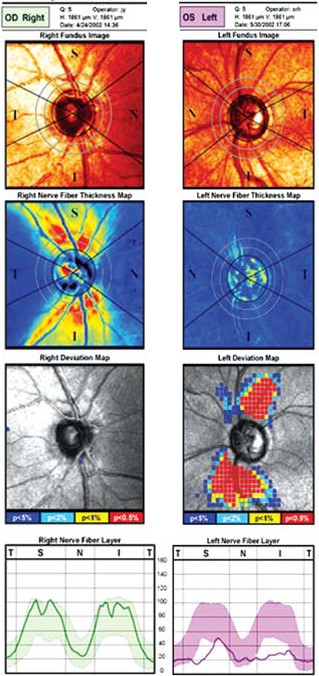
GDx scans of right normal eye and left glaucomatous eye showing loss or thinning of the nerve fibre layer. The top image is a photograph of the nerve, the next is a map of the nerve fibre layer thickness, then next is photograph overlaid with colous showing the areas of nerve fibre loss. The botton graph shows the normal (wide band) nerve fibre thickness and the actual thickness measured (thin line). In the left eye the thin line is far below the normal range.
The visual changes caused by glaucoma are typically of increasing loss of peripheral vision, At its worst, it can become ‘tunnel vision’. People with glaucoma often only realize they have lost vision if the damage affects the very central vision, i.e. end stage glaucoma.
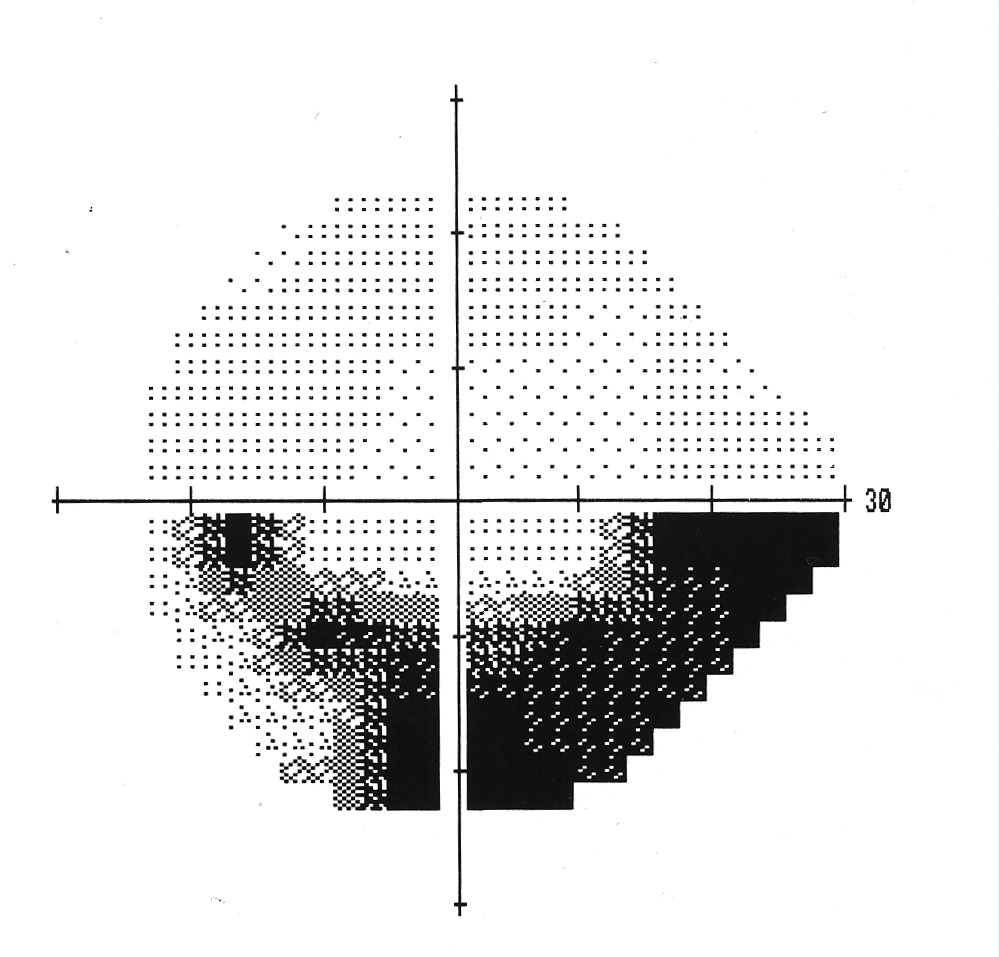
A visual field (test of peripheral vision). The centre of the cross is the central vision. There is an arc-shaped blind curving underneath the central vision. This is typical of glaucoma.
Whilst the underlying cause of glaucoma is unknown, the only known treatment for Glaucoma is to lower the eye pressure. Even if the eye pressure is normal before treatment, lowering the pressure can reduce the progression of glaucoma.
Eye pressure can be lowered in a number of ways, from eye drops, to laser of the trabecular meshwork, insertion of a bypass stent into the trabecular mesh (i-stent), or as a last resort a trabeculectomy, whereby a hole is made into the eye for fluid to slowly leak out via an alternative route.