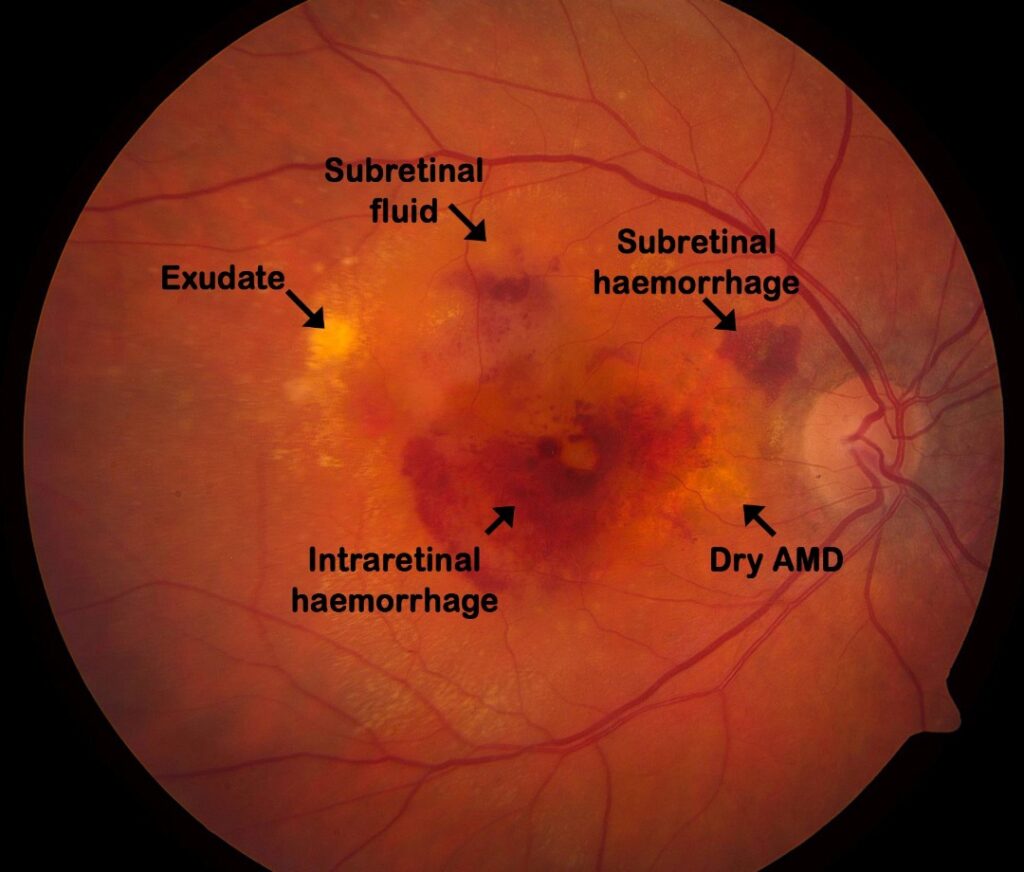
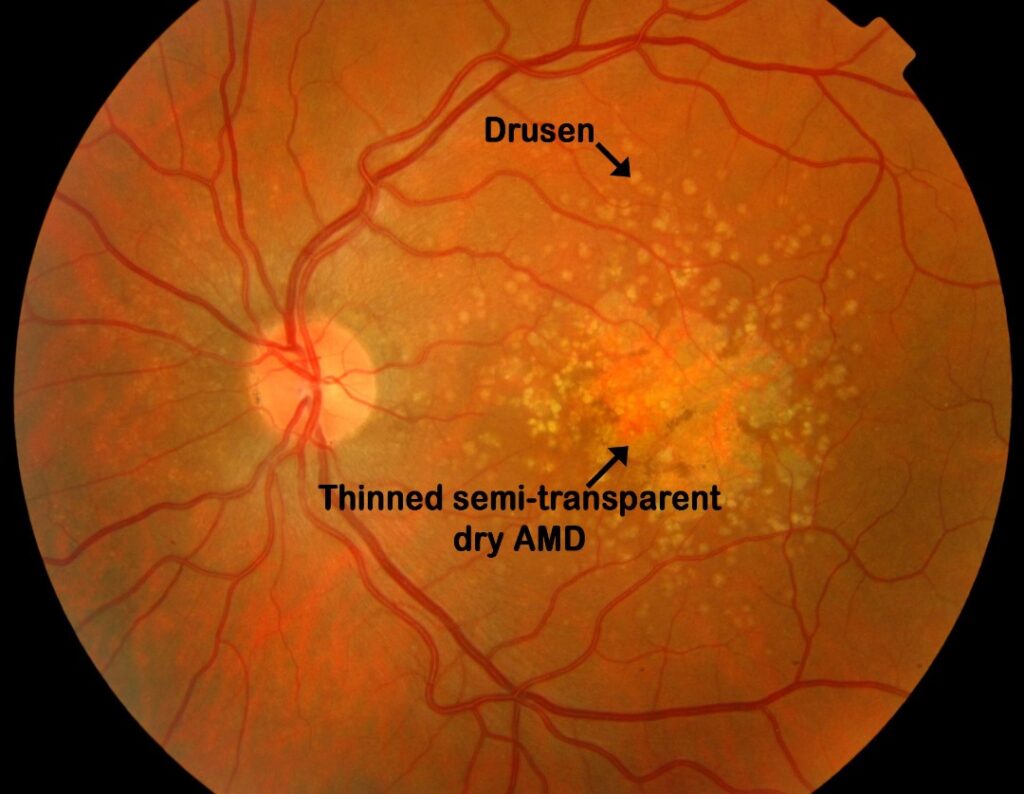
- Age-Related Changes (Drusen & Macular Degeneration)
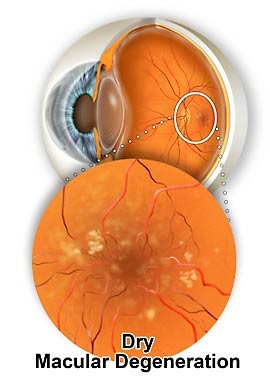
Dry macular degeneration is a gradual wear and tear or thinning of the retina, rather like a well worn jumper that wears thin at the elbows. This thinning of the retina represents tissue loss, and causes gradually increasing blur and distortion. This may take many years to progress significantly and is irreversible. There is no treatment for dry macular degeneration.
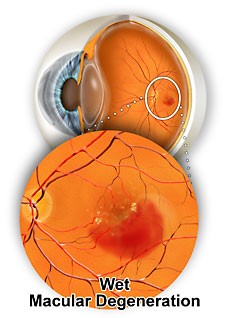
What are the symptoms of wet macular degeneration?
If you are at risk of wet macular degeneration it is important that you monitor your vision for new blur and distortion. This is best done with an Amsler grid on a weekly basis. An amsler is a box full of straight lines. You need to look at the centre of the grid at 30cm with one eye covered. Whilst looking at the centre spot you will notice that around the spot some of the lines may be blurred or distorted (see below).
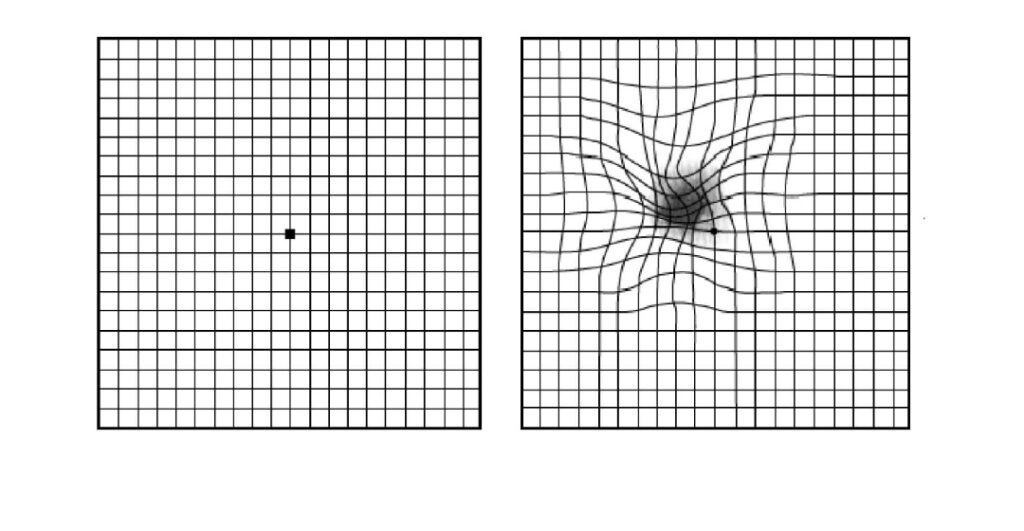
A normal amsler grid on the left. A distorted amsler grid on the right. This is how the grid might look with macular degeneration.
People with longstanding dry macular degeneration may notice distortion on this grid, but this distortion should change very little over months to years. Wet macular degeneration on the other hand is a sudden change to the blur and distortion. If you notice any significant change then you should have your macular examined by an ophthalmologist urgently (within 1 week).
It is important to note that dry macular degeneration can turn into wet macular degeneration. If you are aware of sudden blur and distortion then you need to be seen within 1 week to rule out wet macular degeneration. With modern treatment wet macular degeneration can be stabilised in 95% and improved in 30%. 5% of people with wet macular degeneration get worse irrespective of treatment.
What is the treatment of wAMD?
The treatment of wet macular degeneration is a series of injections into the eye. These injections are initially 4 weekly for 12 weeks. This is known as the loading phase. After this loading phase further injections are based on the response of the macular degeneration, as determined by vision and imaging with OCT. Some people require injections every 4 weeks for years, and others require only the loading dose of 3 injections. Most people are somewhere in-between.
The injectable drugs are known as Avastin (Bevacizimab), Lucentis (Ranibizumab) or Eylea (aflibercept). They are anti vascular growth factors (anti-VEGF) and have an action that blocks blood vessel growth and reduce blood vessel leakage.
Is there anything that I can do to stop AMD getting worse?
The biggest risk factors of AMD is age and genetics. These are not reversible. The most important intervention would be if you were a smoker. Smoking increases your risk of macular degeneration significantly. Other than smoking, the only other changes that can be made are dietary. A good diet rich in leafy green vegetables and fish is protective.
We have good evidence that very high doses of vitamin supplements can slow the progression of both wet and dry macular degeneration significantly. The doses involved are much higher than the amounts that can be achieved through normal healthy eating. The evidence comes from large trials involving many thousands of patients with early macular degeneration. These studies are the Age Related Eye Disease Study, abbreviated ‘AREDS’. The latest trial is called AREDS 2. More than 4,000 people, ages 50 to 85 years, who were at risk for advanced AMD participated in AREDS2. After 5 years they were found to be 25 to 30 percent less likely to develop advanced AMD with this formula.
If you are going to use supplements, then buy supplements that have evidence, and use the AREDS formula:
- 500 mg vitamin C
- 400 iu vitamin E
- 10 mg lutein
- 2 mg zeaxanthin
- 80 mg zinc
- 2 mg copper
Warning: If you are an ex-smoker of less than 15 years, use the formulation that does not contain b-carotene.